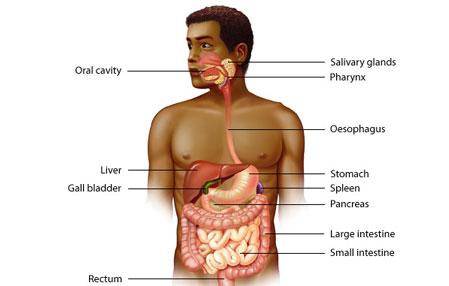
Gastrointestinal oncology (G.I. oncology)
Includes oesophageal and intrabdominal cancers particularly cancers of liver, pancreas, biliary, gall bladder and luminal cancers of oesophagus, stomach, colon and rectum.

Most commonly includes hepatocellular carcinoma (HCC) and liver metastasis from colon or rectal cancers. Intrahepatic cholangiocarcinoma are now being commonly seen. Most common symptoms are fatigue, loss of appetite and weight loss. Liver cancers are mostly diagnosed with triple contrast CT scan of abdomen. In most patients surgery offers long term relief. The most commonly performed surgery is partial excision of liver called right or left hepatectomy. In cases were cancer is limited to left lateral segment of liver a left lateral segmental excision of liver is performed laparoscopically with excellent results. In most cases of liver mets we do laparoscopic metastatectomy. Even with removal of 60% of liver the liver regains its normal volume within 2 weeks, so a major liver resection of 60% can be done safely in most patients. In cases were surgery cannot be performed initially the option is to give TACE (transarterialchemoembolisation) initially which shrinks the tumor followed by surgical excision.
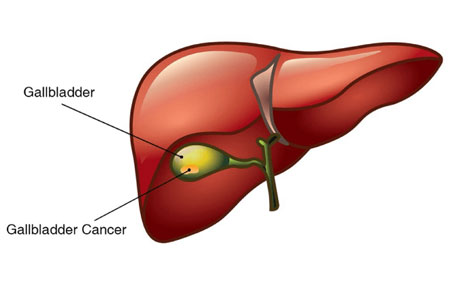
Long standing gall stones predisposes to GBC. Symptoms are mostly continuous pain right upper abdomen, weight loss, loss of appetite. In patients were gall bladder cancer present with jaundice its usually an advanced stage. Stage of disease is best assessed with MRI/ CT of abdomen and at times PET scan is required. Intraoperative ultrasound helps in decision making for margin of excision. Surgery is best treatment modality for GBC. Most commonly performed surgery at our centre is laparoscopic/ open extended cholecystectomy with hepatoduodenal lymph node dissection. CBD excision with hepaticojejunostomy is at times necessary to obtain negative margin. Surgery offers excellent long term relief in patients with early stage of disease.
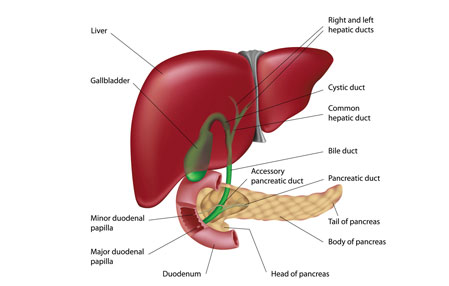
Is being increasingly seen. It is predisposed in patients with choledochal cyst of bile duct, primary sclerosing cholangitis (PSC), ulcerative colitis etc. Symptoms are similar to gall bladder cancer except that jaundice is seen in early course of disease. Bile duct starts from liver and ends into pancreas. Upper end cholangiocarcinoma behaves as liver cancer and lower end behaves as pancreatic cancer. Surgery offers long term relief in patients were it is performed earlier. We at our centre do whipple PD (pancreaticoduodenectomy) for lower bile duct cancers and local excision for mid CBD tumor. Cholangiocarcinoma invading unilateral secondary biliary radicle we perform a standard right or left hepatectomy.
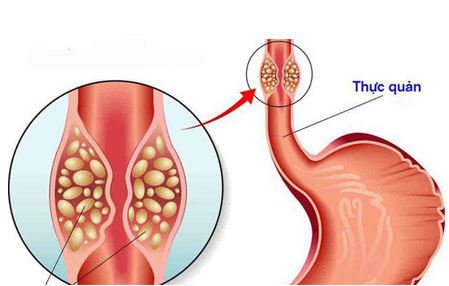
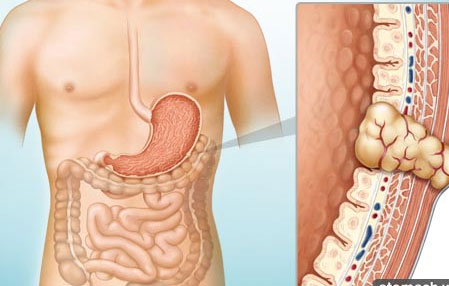
Hot beverages, caustic burn, smoking alcohol and reflux esophagitis predisposes to esophageal cancers. The most common type of esophaeal cancers are adenocarcinoma and squamous cell carcinoma. They are usually diagnosed with upper GI endoscopy and biopsy. At our centre we manage oesophageal and gastric cancers with MDT (multidisciplinary team) which comprises of Gastrosurgeon, Radiation oncologist, Medical oncologist, Gastroenterologist and Radiologist. Surgery offers excellent long term result. At our centre we do most of esophageal surgery by laparoscopic/ minimal invasive method commonly known as thoacoscopicesophagectomy or VATS (video assisted thoracoscopic surgery). In cases were tumor is advanced surgery is done by open method thoracotomy or open abdominal approach.
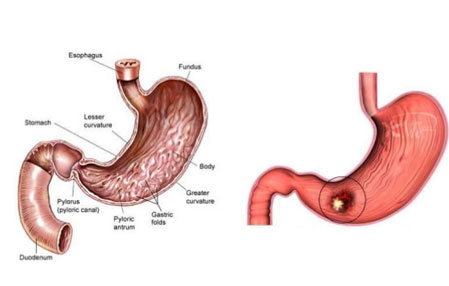
Gastric cancers usually present with loss of appetite, weight loss, blood in vomitus, pain abdomen, anaemia and weakness. Smoked food, alcohol, tobacco and smoking increases risk of gastric cancers. Adenocarcinoma is most common type gastric cancers. Diagnosis is confirmed with endoscopy and biopsy. Surgery (Gastrectomy) with lymphadenectomy (lymph nodes excision) offers long term relief. Gastrectomy with D2 lymphadenectomy stands the current standard of care for surgery in gastric cancers. Gastrectomy can be total or distal (partial) depending on stage and location of tumor. Total gastrectomy with D2 lymphadenectomy with Roux en y esophagojejunostomy is done for proximal gastric cancers.

GEJ cancers hold a special subset of gastric cancer as lies at junction of esophagus and stomach. The management of GEJ growth depends on type and extent of cancer invasion into esophagus and stomach.
GIST ranges from benign to malignant potential. GIST can occur anywhere from stomach , intestine to colon. Gastric GIST are most common. Surgery is curative treatment in most cases. We perform most of GIST surgery by laparoscopic method. Post surgery (GIST excision) if required oral drug like imatinib offers long term relief.
Are slow growing tumors and can occur anywhere from stomach, duodenum, small intestine or colon. Surgery combined with chemotherapy offers long term relief. Most surgical excision of lymphomas are possible with minimal access surgery.
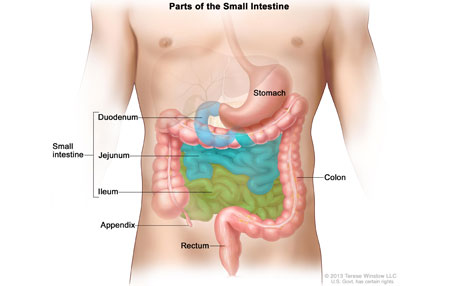
Are relatively uncommon. Most common are duodenal malignancy followed by adenocarcinoma of small bowel. Local excision and anastomosis (resection anastomosis) is most commonly performed.
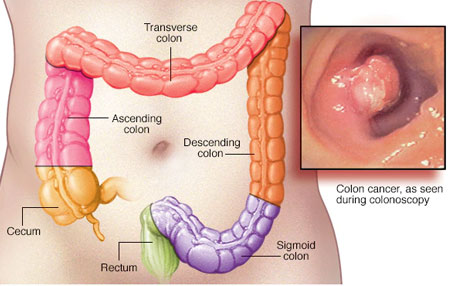
Can be in any part of large bowel from caecum to rectum. Most common symptoms of colonic cancer are blood in stool. Prognosis is good if treatment is given in early stage of disease. Diagnosis is usually made with colonoscopy and biopsy. Adenocarcinoma of colon is most common colon malignancy. Laparoscopic surgery is now standard of care for colonic cancers. The most commonly performed surgery are right hemicolectomy for right colonic cancers and anterior resection for left sided colonic cancers.
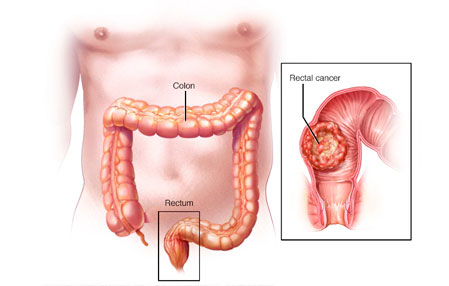
Rectum extends from upper margin of anus to recto-sigmoid junction. Cancer in rectum presents with constipation and bleeding per rectum. Digital rectal examination, proctoscopy and biopsy in OPD at times diagnostic. Management of rectal cancers involve MDT with Gastrosurgeon, Radiation oncologist, Medical oncologist and Radiologist. Radiation therapy is at times preceded by surgery and can preserve normal continence even in low rectal cancers. Most common surgery performed for rectal cancers are low anterior resection, ultra low anterior resection, abdominal perineal resection (APR) and pelvic exenteration. Low anterior resection with total mesorectal excision (TME) is standard of care for rectal cancer and can be performed laparoscopically in most cases. APR and Pelvic exenteration are morbid procedure where a neo opening is fashioned from abdomen for defecation.
Retroperitonealsarcomas orleiomyomaslies in retroperitoneal space and is managed with surgery and chemotherapy.
